You are not imagining the contradiction
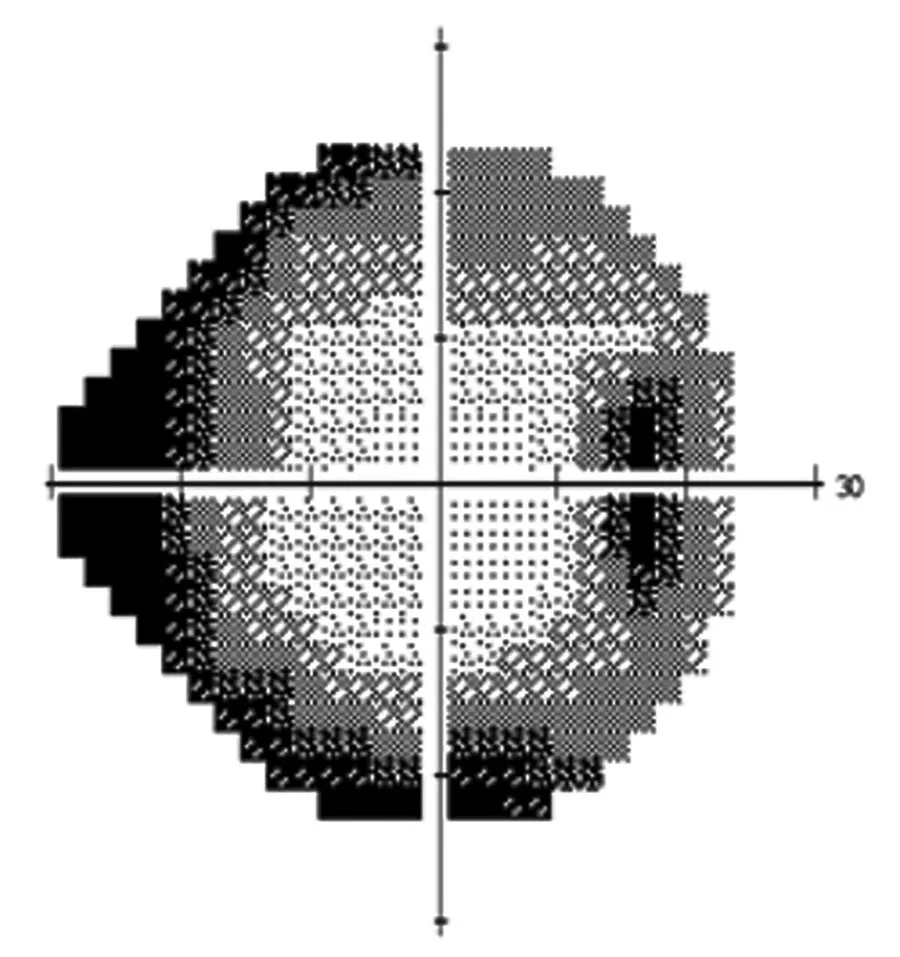
Your eye pressure may be at target, your injections may be on schedule, or your blood sugar may be better controlled - and yet your visual field, OCT, contrast sensitivity, night vision, or reading ability may still be declining. That does not automatically mean your treatment has failed. It means your disease, your treatment response, and the condition of the remaining visual tissue need to be reassessed carefully.

.webp)